End tidal CO2 monitoring is represented as a number and a graph on a monitor. The number is called capnometry, which is the partial pressure of CO2 detected at the end of exhalation, ranging between 35 – 45 mm Hg or 4.0 – 5.7 kPa. The waveform is called capnograph and shows how much CO2 is present at each phase of the respiratory cycle.
End tidal CO2 (EtCO2) monitoring is the fastest indicator of ventilatory compromise. Whilst capnography assesses ventilation, which is the movement of air in and out of the lungs; pulse oximetry assesses oxygenation which is the amount of oxygen that is bound to red blood cells.
TYPES OF END TIDAL CO2 MONITORS
There are 3 main types of End Tidal CO2 monitors: sidestream, main¬stream, and Microstream.
Sidestream monitors rely on a separate monitor connected to the patient’s airway by a tube. Gas samples are aspirated from exhaled gas flow via the ventilator circuit and are read at the monitor. Sidestream monitors can be used with non-invasive ventilation.
Mainstream monitors have a sampling window which is inserted directly in-line with the ventilator circuit for CO2 measurement. This allows a more rapid response time and requires a smaller amount of sample gas than sidestream monitoring. But mainstream monitors increase mechanical dead space, depending on size of the chamber used to collect a gas sample, while adding weight on the airway, and can’t be used for non-invasive ventilation.
The newest type of EtCO2 monitor is Microstream which uses molecular correlation spectrography for greater precision. The Microstream monitor has a rapid response time and may be used with both invasive and non-invasive ventilation.
HOW TO INTERPRET END TIDAL CO2 MONITORING?
When monitoring End Tidal CO2, there are 3 aspects to consider: the EtCO2 value, the waveform shape and the respiratory rate (RR). Whilst it is fairly easy to interpret numerical values for EtCO2 and RR, interpretation of the waveform shape requires specific knowledge discussed below.
A normal capnogram always has the following features:
The waveform shape always starts at zero and returns to zero
A maximum CO2 is reached with each breath, corresponding to EtCO2
The amplitude of the waveform depends on EtCO2 concentration
The width of the waveform depends on expiratory time
There is a similar shape for subjects with normal lung function
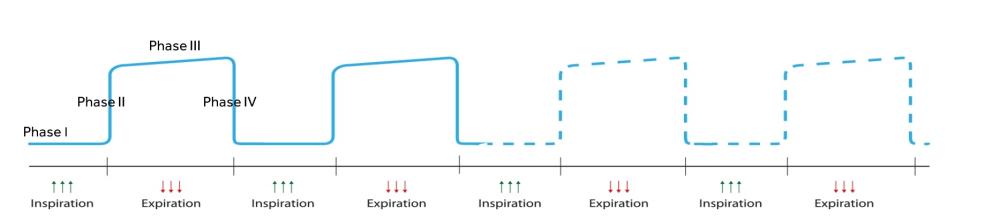
The waveform has four phases:
Phase I: start of exhalation, CO2 concentration is initially zero
Phase II: CO2 increases rapidly as alveolar gas exits the airway
Phase III: CO2 concentration is relatively constant (reflects the concentration of CO2 in the alveolar gas). This phase ends with a value of maximum CO2 concentration
Phase IV: start of inhalation, CO2 decreases to zero as atmospheric air enters the airway
The following image is taken from SedateUK
PROPER
Check if the readings for quantity, rate, shape and trending are normal for that particular patient, considering any metabolic, ventilatory or perfusion problems
QUANTITY
EtCO2 value should be 35-45 mmHg or 4.0 – 5.7 kPa
RATE
Ventilation should be 12-20 breaths per minute (bpm) for adults who are breathing by themselves; and 10-12 bpm if being ventilated. Children should be ventilated at a rate of 15-30 bpm; 25-50 bpm for infants. Ventilating too quickly won’t let enough CO2 build up in the alveolar, resulting in lower EtCO2 readings. Ventilating too slowly will allow extra CO2 to build up, resulting in higher readings
SHAPE
Waveform should normally be a rectangle with rounded corners
TREND
Trending of the quantity, rate and shape of EtCO2 should be stable or improving
WHY IS END TIDAL CO2 MONITORING IMPORTANT?
Although it has been historically used by anaesthetist during general anaesthesia, End Tidal CO2 monitoring is becoming more common in other clinical areas like emergency environments, critical care, during sedation practice, in ambulatory settings and in post-operative recovery units. Several guidelines have supported the use of capnography outside the theatre environment:
ALS Guidelines (2015) mention “Waveform capnography must be used to confirm and continually monitor tracheal tube placement, and may be used to monitor the quality of CPR and to provide an early indication of return of spontaneous circulation (ROSC).”
House of Delegates of ASA (2011) “During moderate or deep sedation, the adequacy of ventilation shall be evaluated by continual observation of qualitative clinical signs and monitoring for the presence of exhaled carbon dioxide unless precluded or invalidated by the nature of the patient, procedure, or equipment.”
AAGBI (2015) “Continuous capnography should be used for all patients undergoing moderate or deep sedation, and should be available wherever any patients undergoing anaesthesia or moderate or deep sedation are recovered.”
The wider use of EtCO2 monitoring in different clinical areas reflects its importance as a monitoring tool that gives indication into three crucial aspects: the patient’s airway patency, breathing adequacy and circulatory status. Professionals are able to identify potential breathing complications (such as airway obstruction, hyperventilation, hypoventilation, or apnoea) and respond accordingly with a change in clinical management.3 As it provides real time, ongoing data, it prompts early diagnosis, allowing for clinical interventions to be adjusted according to monitor trends and preventing further deterioration.
In critical care, End Tidal CO2 monitoring is used to assess adequacy of circulation to the lungs, which provides clues about circulation to the rest of the body. Low EtCO2 with other signs of shock indicates poor systemic perfusion, which can be caused by hypovolemia, sepsis or dysrhythmias.1
In cardiac arrest, it is used to indicate effectiveness of chest compressions. An EtCO2 less than 10 mm Hg indicates that compressions are not fast or deep enough. If circulation is restored, a spike in EtCO2 often appears before a pulse is detected. It is also used to confirm endotracheal tube placement and effective ventilation.
In sedation practice, End Tidal CO2 helps professionals assess ventilatory function which is usually impaired by sedative and analgesic medication and allows early detection of respiratory compromise and timely intervention.
Data obtained from End Tidal CO2 monitoring depends on proper equipment function and is only as useful as the clinician’s ability to interpret and apply it. Understanding the key facts highlighted in this article will help you get started with understanding this technology and its implications in clinical practice.